Sciatica: Is It Coming From the Piriformis or a Disc?

"Sciatica" is a symptom, not a diagnosis. The two most common drivers — a lumbar disc irritating a nerve root, and the piriformis muscle compressing the sciatic nerve — behave very differently. Here is what the evidence says, and a few things you can try at home to tell them apart.
Most people who walk into the office saying "I have sciatica" don''t actually know what''s causing it — they know they have pain shooting down the back of the leg. That symptom has two very common sources, and telling them apart matters because the treatment, prognosis, and things you should (and shouldn''t) do at home are different.
The two big culprits: a lumbar disc irritating a nerve root (a true radiculopathy), and the piriformis muscle compressing the sciatic nerve deep in the buttock (deep gluteal syndrome / piriformis syndrome).
First, what "sciatica" actually means
Sciatica is a symptom: pain, numbness, tingling, or weakness following the path of the sciatic nerve — usually buttock, back of thigh, calf, and sometimes foot. Roughly 85–90% of true nerve-root sciatica is caused by a lumbar disc herniation compressing an exiting nerve root, most often at L4–L5 or L5–S1 (Jensen et al., BMJ, 2019). Piriformis-driven sciatic nerve compression is far less common but very real, and it is under-diagnosed on standard MRI because the pathology is muscular, not structural (Hopayian & Danielyan, European Journal of Orthopaedic Surgery & Traumatology, 2018).
The point: you need to figure out which nerve, and where it''s being irritated, before you can pick the right plan.
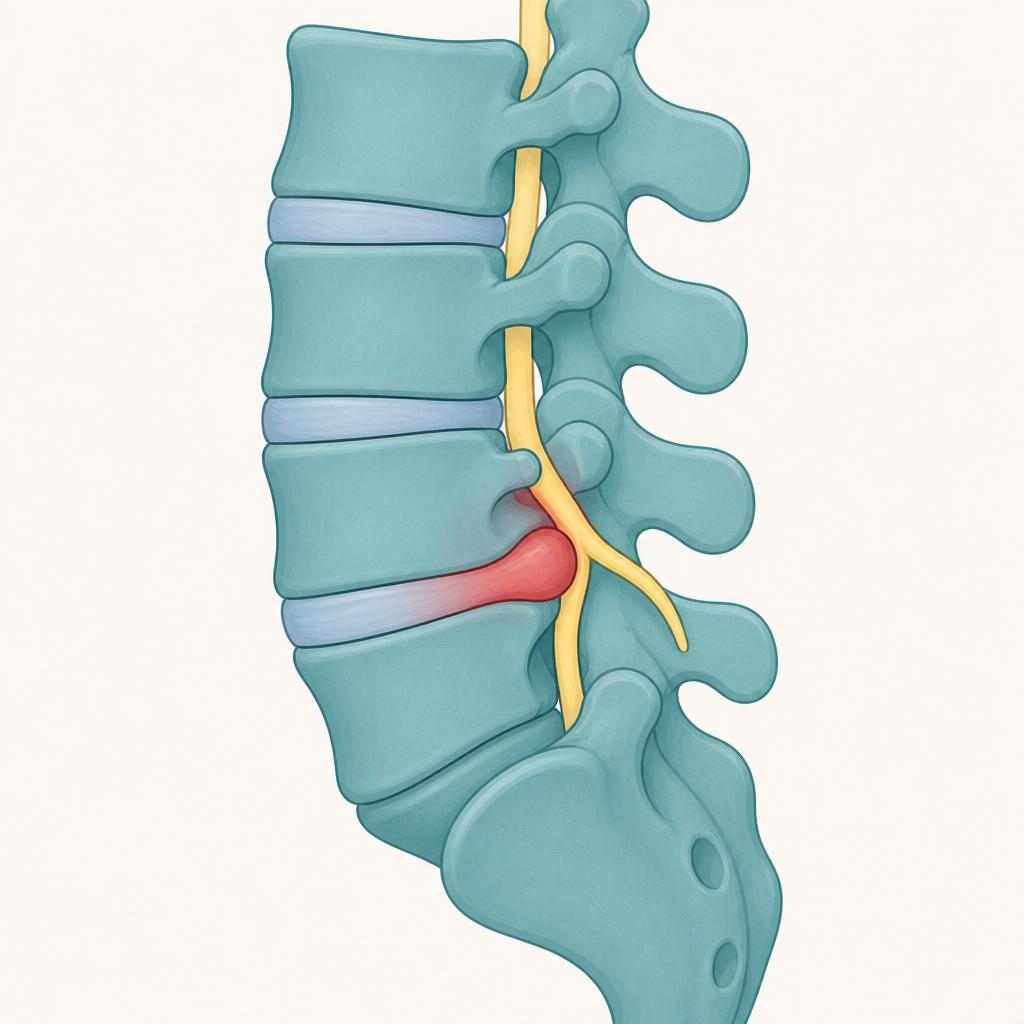
What a disc problem actually does
A lumbar disc herniation compresses or chemically irritates a spinal nerve root as it exits the spine. The classic pattern (Vroomen et al., Journal of Neurology, Neurosurgery & Psychiatry, 2002; NASS Clinical Guidelines on Lumbar Disc Herniation with Radiculopathy, 2012):
- Pain follows a dermatome. L5 sends pain down the outer leg into the top of the foot and big toe; S1 sends it down the back of the calf into the pinky-toe side and heel.
- It is worse with spinal loading. Sitting for long periods, bending forward, coughing, sneezing, or straining on the toilet reliably flare it. That''s because those movements increase intradiscal pressure (Nachemson, Spine, 1981).
- Neurologic signs may show up. Numbness in a specific patch of skin, foot-drop, weakness pushing off the big toe, or diminished ankle reflex all point to a nerve root, not a muscle.
- The straight-leg raise reproduces the leg pain, not just tightness (see the home test below).
- Good news on prognosis: the majority of disc herniations resolve without surgery. Follow-up MRIs show spontaneous regression of the herniated disc in a large percentage of cases, and symptom improvement usually tracks with that (Chiu et al., Clinical Rehabilitation, 2015, meta-analysis).
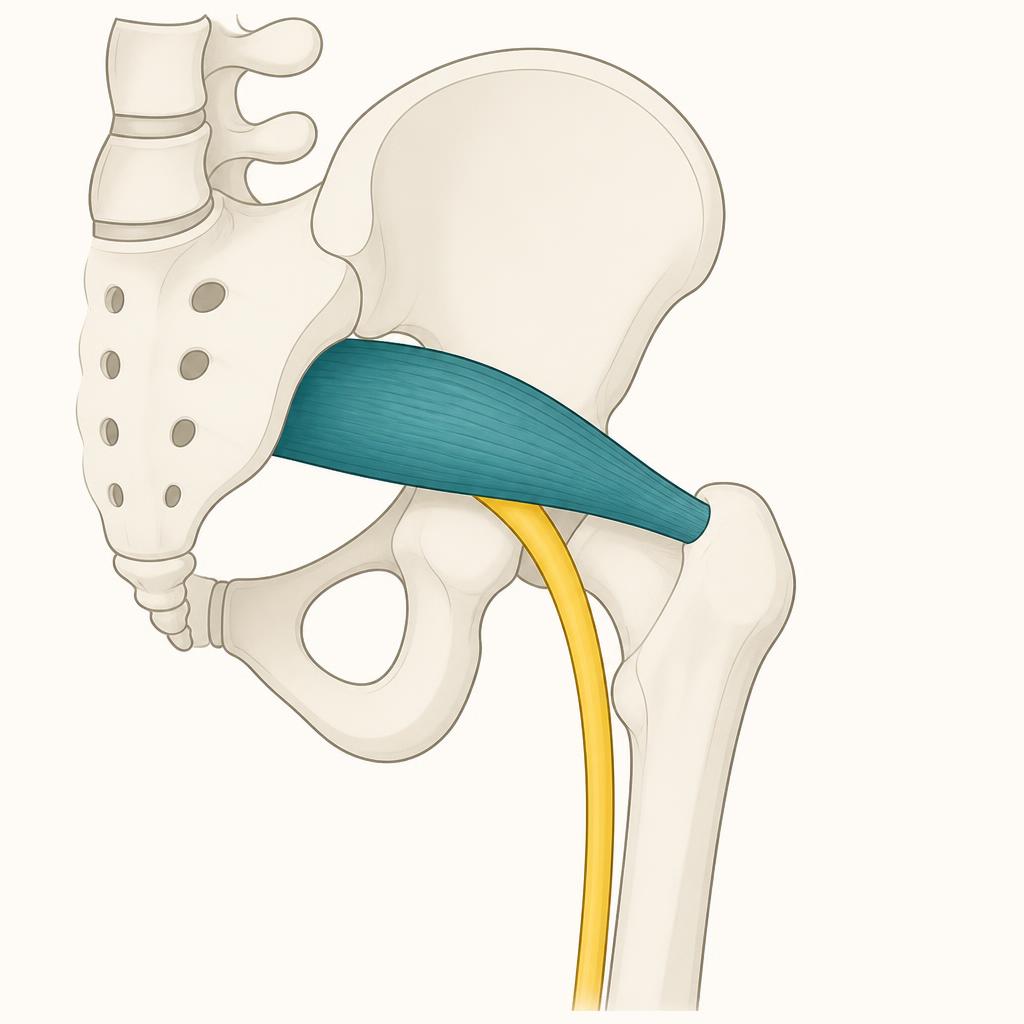
What piriformis compression actually does
The piriformis is a small pear-shaped muscle deep in the buttock. The sciatic nerve runs directly beneath it (and in some people, straight through it). When the muscle is tight, shortened, or in spasm, it can compress the nerve — producing symptoms that look and feel a lot like disc sciatica, but with different triggers (Hopayian et al., European Spine Journal, 2010 — systematic review of piriformis syndrome findings; Michel et al., Anaesthesia, Critical Care & Pain Medicine, 2013).
Typical features:
- Pain is deep in the buttock, often described as "sitting on a golf ball," and only sometimes travels down the leg. When it does travel, it usually stops at the back of the thigh rather than continuing past the knee.
- Sitting on a hard surface, driving, or crossing the affected leg over the other knee flares it. Bending forward to tie a shoe usually does not.
- No true dermatomal pattern, no reflex loss, no weakness — because the nerve is being squeezed in the buttock, not compressed at its root.
- Direct tenderness deep in the mid-buttock (roughly halfway between the sacrum and the greater trochanter) is common; pressing there often reproduces the leg symptoms.
- Hip rotation tests reproduce it, not spinal loading (see the home tests below).
Home tests you can try (safely)
These aren''t a substitute for an exam, but they''re a reasonable way to tell which direction your pain is pointing. Do them once, slowly. Stop immediately if anything gets worse, and see the red-flag list at the bottom before you experiment.
1. Straight-leg raise (points toward the disc)
Lie flat on your back on the floor. Keep the painful leg straight and slowly lift it toward the ceiling, foot relaxed.
- Suggests a disc: familiar shooting/electric pain reproduced down the leg somewhere between about 30 and 70 degrees of lift. Sensitivity for lumbar disc herniation is around 91% (Deville et al., Spine, 2000, meta-analysis).
- Suggests not a disc: only hamstring tightness with no leg pain, or pain that doesn''t appear until you''re nearly vertical.
Bonus: while your leg is at the height that reproduces pain, pull your toes toward your face (dorsiflexion). If that sharpens the leg pain, it strongly suggests nerve-root involvement.
2. Slump test (also points toward the disc)
Sit on the edge of a chair, slump your upper back, drop your chin to your chest, straighten the painful leg out in front of you, then pull your toes toward your face. If this reproduces your familiar leg pain, and lifting your head back up eases it, that''s a nerve-tension pattern most consistent with a disc/nerve-root source (Majlesi et al., JCR: Journal of Clinical Rheumatology, 2008).
3. FAIR test — flexion, adduction, internal rotation (points toward the piriformis)
Lie on your unaffected side. Bring the painful-side knee up in front of you to about 60 degrees of hip flexion, then let the knee drop across your body toward the floor while you rotate the shin upward. If this reproduces deep buttock pain (with or without a little travel down the back of the thigh), it points at the piriformis (Fishman et al., Archives of Physical Medicine and Rehabilitation, 2002).
4. The "sit test"
- Piriformis pattern: sitting on a hard chair is much worse than sitting on a soft one, and the pain is centered in the buttock cheek — because you''re compressing the muscle directly. Standing up briefly relieves it.
- Disc pattern: any prolonged sitting builds up pain and shoots it down the leg, regardless of surface, because sitting loads the disc. Standing up often does not provide immediate relief; walking usually does.
5. The cough/sneeze/strain test
If coughing, sneezing, or bearing down on the toilet sends a jolt down your leg, that''s classic for a disc (it spikes intradiscal and intrathecal pressure). Piriformis compression is essentially never triggered by coughing.
Quick pattern summary
| Feature | Disc / nerve root | Piriformis |
|---|---|---|
| Pain worst with | Sitting, bending forward, coughing | Sitting on hard surfaces, crossing legs, driving |
| Pain travels | Often past the knee, into foot/toes | Usually stops at back of thigh |
| Dermatomal (numb patch, reflex loss, foot weakness) | Common | Rare |
| Straight-leg raise reproduces leg pain | Yes | No (or only mild) |
| Deep buttock tenderness | Sometimes | Almost always |
| Cough/sneeze reproduces it | Yes | No |
What to do at home while you sort it out
If it looks like a disc, the evidence supports staying gently active, avoiding prolonged sitting, and doing directional preference movements — for many people that means gentle backward-bending (prone press-ups) and short frequent walks. Bed rest actively slows recovery (Dahm et al., Cochrane Review, 2010). NSAIDs give modest short-term relief; opioids do not out-perform them and carry more risk (Qaseem et al., Annals of Internal Medicine, 2017 — ACP guideline).
If it looks like piriformis, targeted stretching of the piriformis (figure-4 stretch, supine knee-to-opposite-shoulder), soft-tissue work on the buttock (a lacrosse ball against a wall, one to two minutes, not aggressive), and getting out of prolonged sitting every 30 minutes are all reasonable first steps (Boyajian-O''Neill et al., Journal of the American Osteopathic Association, 2008; Tonley et al., Journal of Orthopaedic & Sports Physical Therapy, 2010). Fixing gluteus medius weakness — the underlying cause in a lot of piriformis cases — is the piece that keeps it from coming back.
Either way, motion is the treatment, not rest. Prolonged bed rest makes both worse.
When it''s not something you should self-manage
Skip the home experiments and get evaluated urgently if you have any of these:
- Loss of bowel or bladder control, or a new numb saddle-shaped patch between your legs — possible cauda equina syndrome, a surgical emergency.
- Progressive weakness — a foot that''s getting harder to lift, or a leg giving way.
- Pain following recent significant trauma, a history of cancer, unexplained weight loss, night sweats, or fever with back pain.
- Symptoms in both legs at once.
- Pain that''s been getting steadily worse for more than 6 weeks despite reasonable self-care.
None of the above are common — but they''re the ones you don''t want to miss.
Bottom line
"Sciatica" tells you the sciatic nerve is angry. It doesn''t tell you where it''s angry. A disc irritates the nerve at its root and gives you dermatomal pain that hates sitting, bending, and coughing. A tight piriformis pinches the nerve in the buttock and gives you deep local pain that hates hard chairs and crossed legs. A few well-chosen tests at home will usually point you in one direction — and that direction should drive what you do next.
If you''re not sure, or if home care isn''t moving the needle in two to three weeks, come get an exam. It''s a 20-minute question to answer in person, and the right answer changes the plan entirely.